
Return on Patience
Ninety miles. Twelve years. And the wrong kind of money.


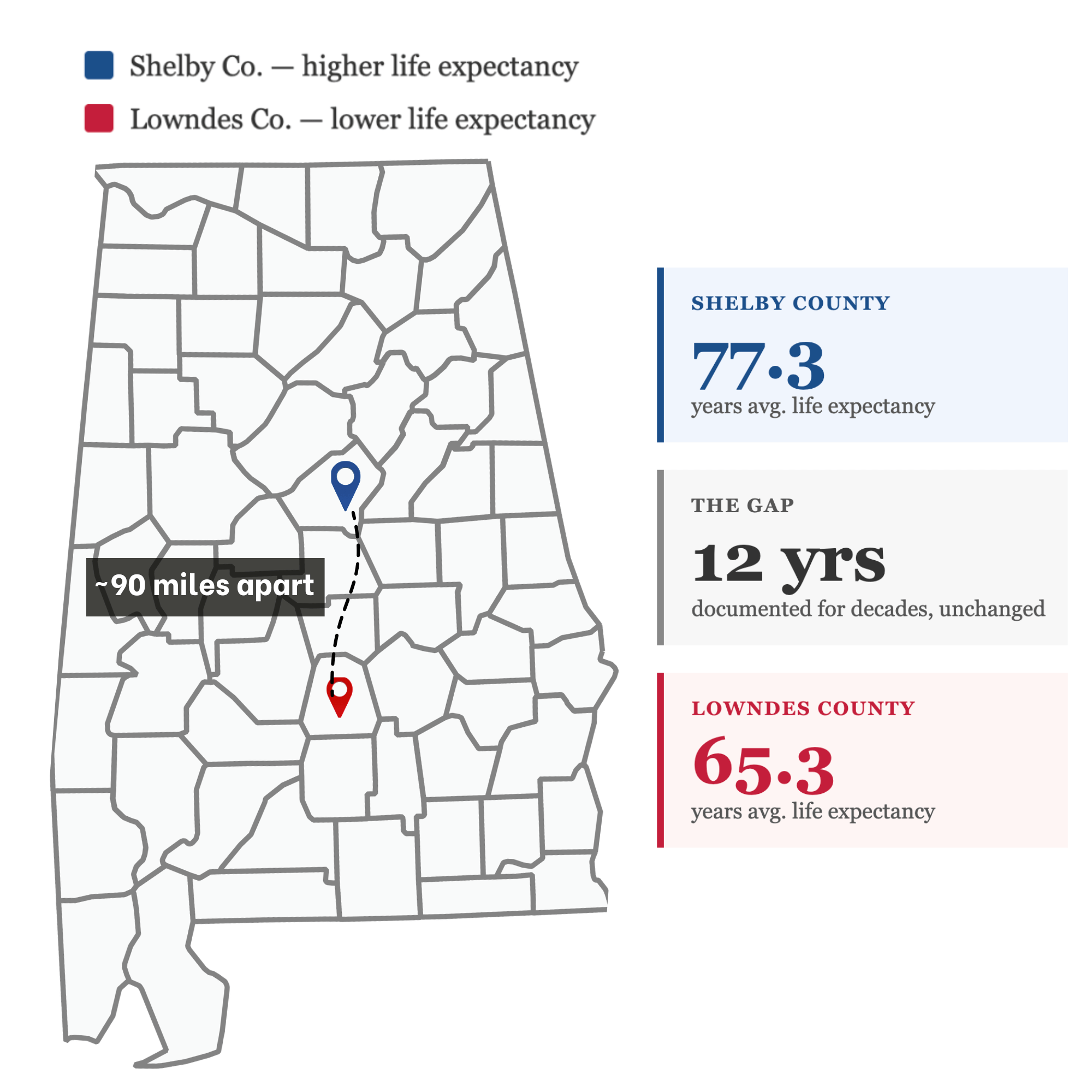
Lowndes County and Shelby County are ninety miles apart. They share a state, a healthcare system, a governor, and a set of federal health programs that apply equally to both. What they don’t share is life expectancy. Shelby County residents live, on average, twelve years longer.
Twelve years. The gap between a grandmother who watches her grandchildren graduate and one who doesn’t. A man who retires and one who doesn’t make it there. And this isn’t an anomaly; it’s the map of Alabama, county by county.
Alabama’s health crisis has been documented since before most of us were working in this industry. Reports have been written. Task forces convened. Federal dollars allocated. The gap still has not closed.
We want to make an argument about why. And it isn’t the argument you’ve probably heard.
The prevailing assumption is that Alabama has a healthcare delivery problem: not enough providers in rural counties, not enough access. And how do we fix this? With capital. Capital to attract doctors and keep rural hospitals open. Grants to fund initiatives. Expand Medicaid. Get Medicare or private insureres to pay more per service.
Yes, we need capital and…
we need to think differently about how we deploy that capital.
That’s because it will take a really long time for us to get enough grants and tax-payer dollars and higher premiums to solve the problem.
To improve our health quickly, we need to invest capital differently.
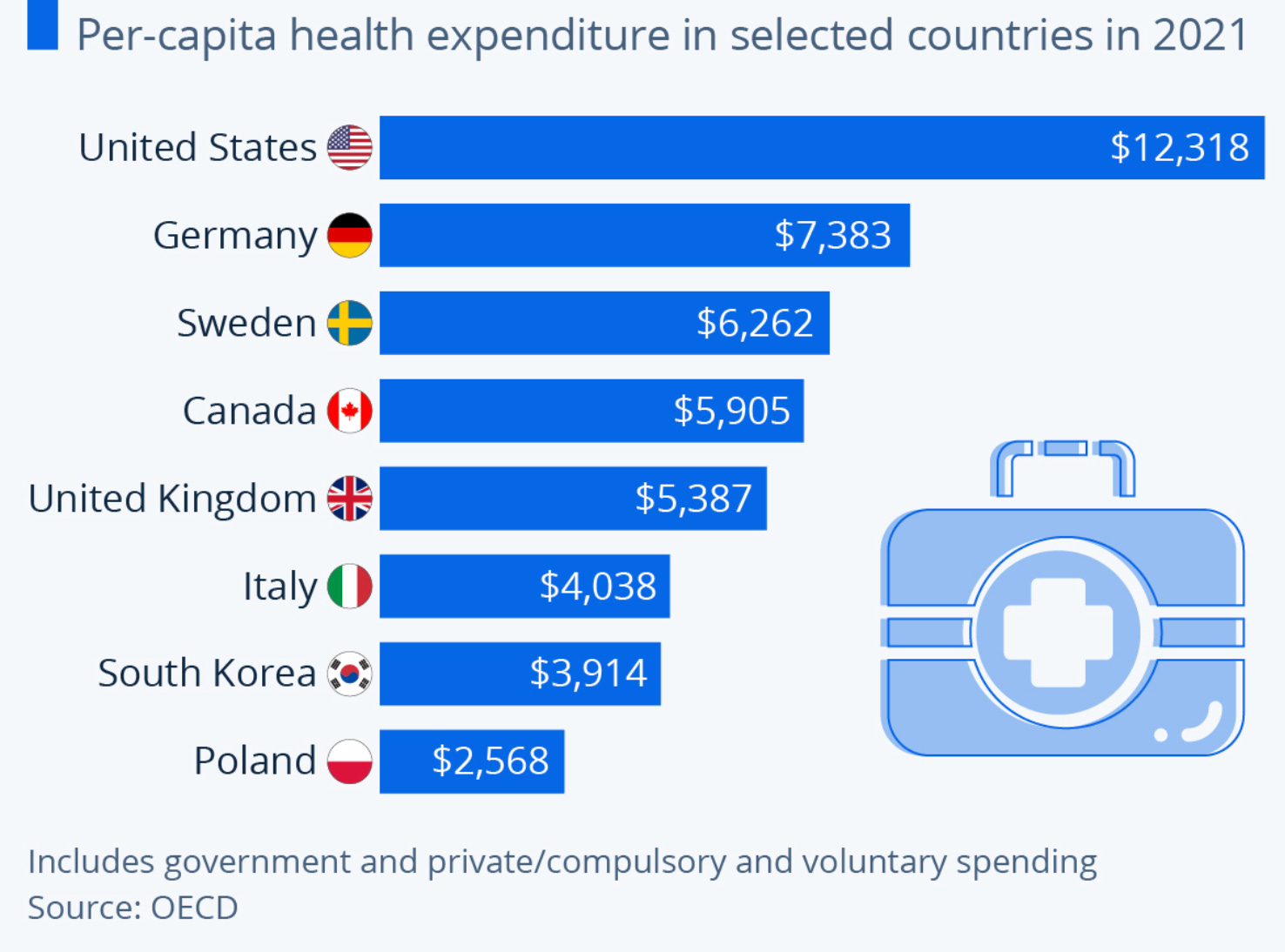
We know that other nations spend less per capita than we do on health (Lowndes county included) and consistently get better outcomes. The interventions that have moved health outcomes most in human history weren’t expensive: antibiotics, clean water, flushing toilets. Low-cost, unglamorous, and transformative. What Alabama needs isn’t just more money or technology to fix the problem; it needs capital built for the kinds of solutions that actually work here.
Low-cost, unglamorous, and transformative.
The problem is that the capital structures we use to fund healthcare innovation were engineered for a completely different kind of problem, and that mismatch is doing real damage that rarely gets addressed directly. When you apply the wrong instrument to a problem long enough, not only do you fail to solve it, you make it harder to solve.
Venture capital was built for a specific kind of company, one that can go from zero to a billion in five years and scale without asking permission. In healthcare, permission is the whole job.
That structure produced the internet economy, the mobile economy, and a lot of genuinely valuable things. In healthcare, it’s producing something different.
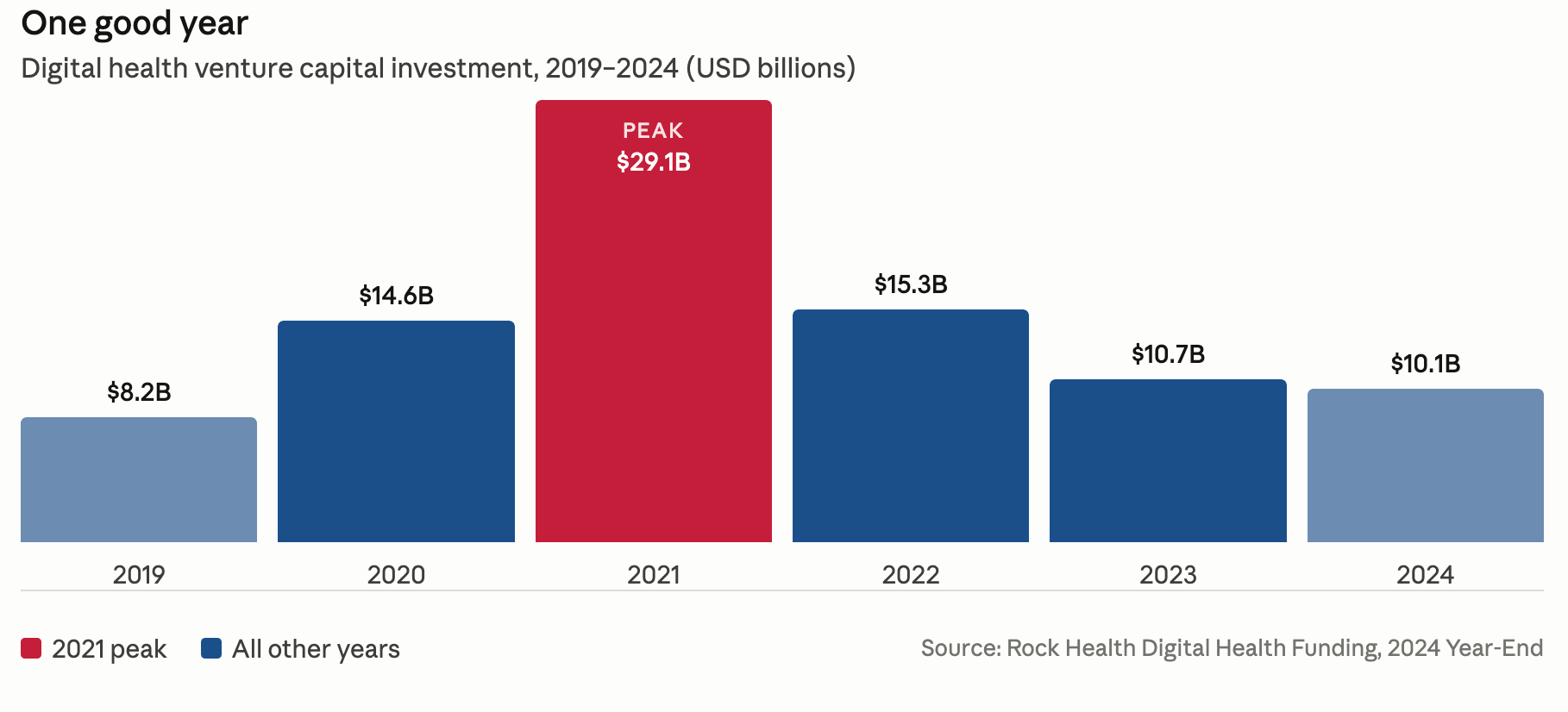
Between 2020 and 2022, digital health attracted an unprecedented wave of venture capital: over $29 billion at its peak.¹ What followed was a slow-motion collapse that should have started a more serious industry conversation than it did. Some examples:
Babylon Health raised over $1 billion, went public at a $4.2 billion valuation, and was delisted within two years.
Olive AI raised $902 million to automate hospital operations and shut down in 2023.
Bright Health raised $1.9 billion and exited five states in a single year before the business failed entirely.
These weren’t bad ideas. Several of them were built around real problems. What killed them was the structural mismatch between what they were trying to build and the timelines their capital demanded.
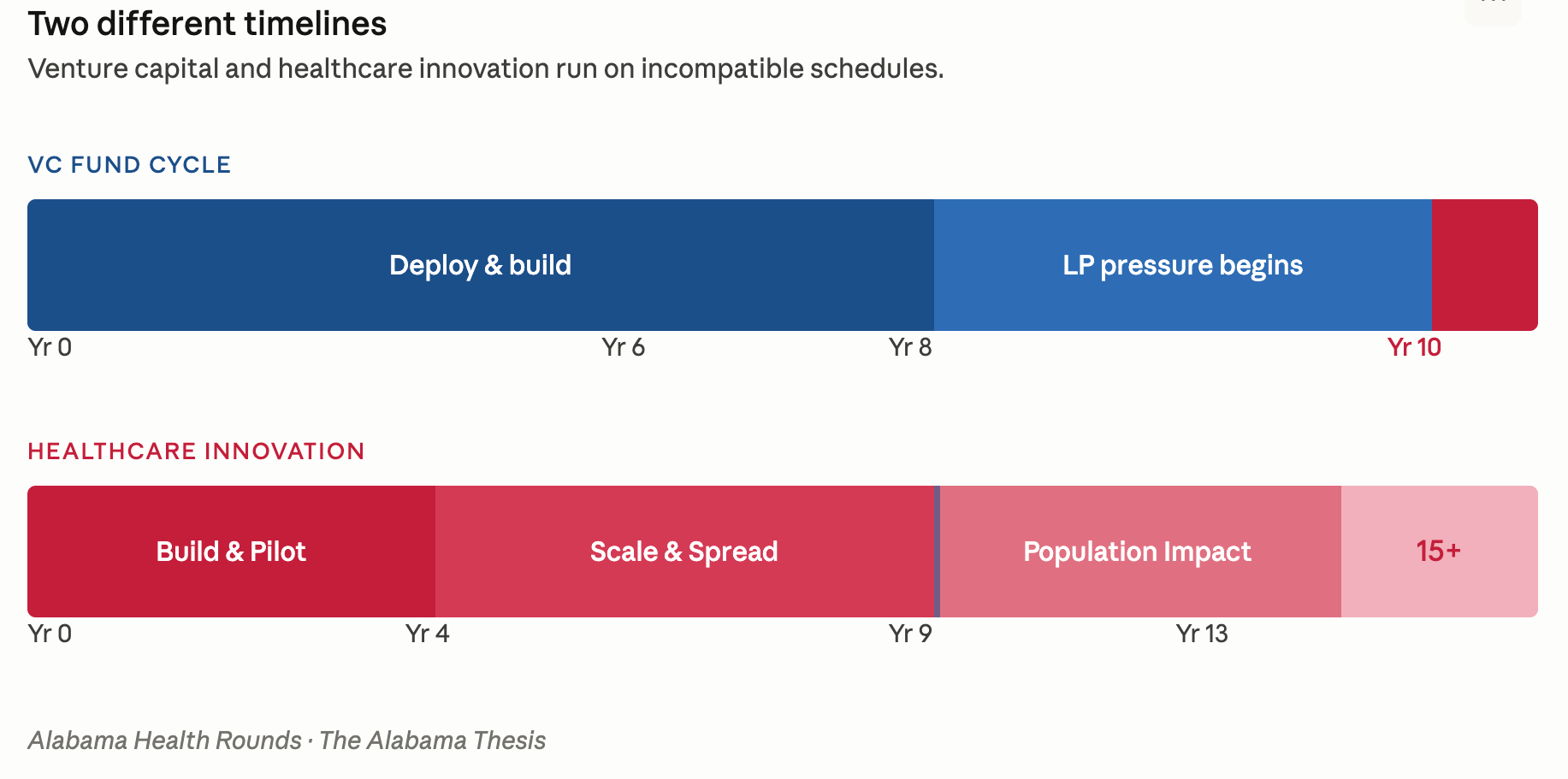
Healthcare doesn’t let you ship, learn, and exit in five years. Care delivery transformation can take a generation. The preventive health infrastructure that actually decreases cost e.g. community health workers, care navigation, behavioral health integration, the upstream interventions that keep people out of emergency rooms, takes years to produce outcomes at a scale that satisfies a fund’s return schedule.
When you force those timelines together, founders feel the pressure whether or not anyone says it out loud. They optimize for what converts in a demo instead of what changes behavior over five years. They chase customers who close fast instead of communities that need them most. At the portfolio level, power law logic shapes (read: distorts) the kinds of companies that get built.
To improve health dramatically, Alabama doesn’t need moonshots. What good is a unicorn if someone in Lowndes County is still choosing between their blood pressure medication and their phone bill?
The companies healthcare actually needs are systems builders: slower, harder to categorize, built around the unglamorous work of making care reach people who need it. They almost never survive a conventional fund cycle.
Instead, capital flows to legible problems that can demonstrate growth metrics investors already know how to read. Oncology platforms. Digital front doors. Prior authorization automation. Real problems, all of them, and they’ll keep attracting capital because the category is familiar.
The interventions with the most actual leverage in health don’t look like that. They live where behavioral health meets primary care, where social determinants meet clinical intervention, where a community health worker and a county health department and a self-insured employer all need to be part of the solution at the same time. These opportunities span multiple systems, don’t fit in neat SaaS categories, and don’t produce an exit in seven years. So they don’t get funded.
In Alabama, this plays out in concrete terms. The interventions with the most potential e.g., a cardiologist rotating through Lowndes County three days a week, or a care navigator funded by employers whose workforce health costs are driving their margins, can’t access conventional venture funding because their returns are measured in avoided hospitalizations and population outcomes, not multiples. And philanthropy, while valuable, doesn’t build the sustained infrastructure that survives a single grant cycle.
We have unintentionally built a capital ecosystem perfectly aligned with the wrong outcomes. Then we look at the map; Lowndes County, Shelby County, ninety miles, twelve years and wonder why nothing has moved.
A different approach requires investors who came in knowing the context.
Patient capital aligned with healthcare looks like a structure where the investment timeline is built around the actual pace of healthcare transformation from the start. That means investors who understand the compounding happens later and, when it does, it tends to be larger than conventional healthcare VC has been positioned to capture. That’s a different LP conversation than most healthcare funds are having. It’s also the only one that makes sense for the problem.
It means going beyond the familiar to fund the interventions most funds won’t; like the multi-stakeholder, cross-system plays that are hard to categorize, hard to pitch, and have been avoided by capital precisely because of their complexity. In healthcare, what looks “unscalable” to traditional VC often describes the opportunities that actually work. Healthcare companies fail for a lot of reasons. Rarely is it because the science or technology was wrong. Usually it’s because they hit a system they, both founders and investors, weren’t prepared for.
Alabama is where this gets tested.
Not just because it’s the most resource-constrained market in the country, though it competes for that title; because solving the problem here, with this history and this level of capital avoidance and this twelve-year life expectancy gap between two counties you can drive between in under two hours, is a different kind of proof than solving it somewhere easier. If a different capital structure can move outcomes in Lowndes County, it can move them anywhere.
As goes healthcare in the Deep South, so goes the nation.
The money is there. What’s been missing is a structure that doesn’t mistake a long proof timeline for a failing investment.
And, we think someone should build it.
¹ Rock Health, Digital Health Funding: 2022 Year in Review. rockhealth.com
29% poverty rate in lowndes county as well is a huge drag on healthcare providers. Thank you for such a thoughtful discussion on how to win in the long run.